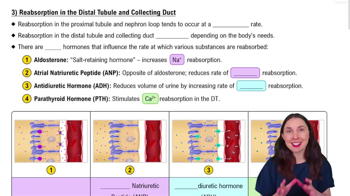
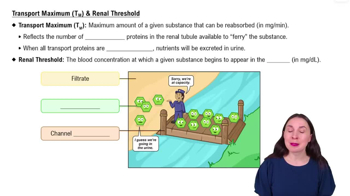
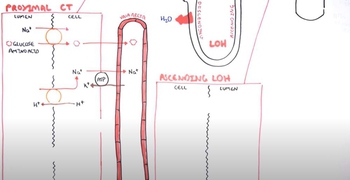
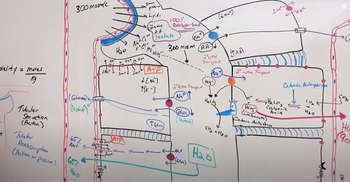
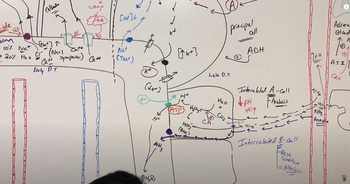
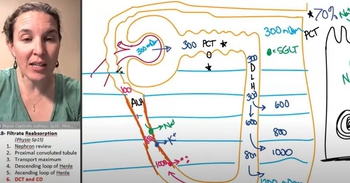
The permeability of the principal cells to sodium ions and water is controlled by two hormones: aldosterone from the adrenal gland, and antidiuretic hormone, or ADH, from the posterior pituitary gland. Let’s first look at the role of aldosterone, which precisely regulates the final amount of sodium reabsorbed. When levels of sodium and potassium ions in the blood are balanced, aldosterone levels remain low. As a result, there are few sodium-potassium ATPase ion pumps in the basolateral membrane and few sodium and potassium channels in the luminal membrane. Therefore, sodium ion reabsorption and potassium ion secretion are both low. However, a decrease in the level of sodium ions or an increase in potassium ions in the blood will trigger the release of aldosterone. Let’s see the results of increasing the level of aldosterone in these cells. In response to increased aldosterone, both sodium ion reabsorption and potassium ion secretion increase. This occurs because the principal cells increase the number and activity of sodium-potassium pumps in the basolateral membrane. The number of sodium and potassium channels in the luminal membrane is also increased. Notice the absence of potassium channels in the basolateral membrane. Potassium ions enter the cell through the basolateral membrane, but instead of diffusing back into the interstitium, the diffuse to the luminal membrane and are secreted into the filtrate. The effects of aldosterone are not confined to the collecting duct. It has similar effects on cells of the distal convoluted tubule. You should also notice the resulting increase in interstitial osmolarity. Water is not following the solute because the luminal membrane of the collecting duct is relatively impermeable to water unless it is stimulated by ADH. Aldosterone and antidiuretic hormone act independently to regulate salt and water, but can also work together. The cell you see here has been stimulated as yet only by aldosterone, so it is still impermeable to water. Let’s see the effect of the pituitary gland releasing ADH. When stimulated by ADH, principal cells quickly insert luminal water channels increasing their water permeability. Notice that the interstitial osmolarity decreases. When water molecules can diffuse through a membrane, osmolarities on each side of the membrane equilibrate. Using this schematic diagram let’s review how filtrate concentration in the tubules is related to interstitial osmolarity. Watch the changes in the concentration and volume of the filtrate as it passes through the differing osmotic environments of the cortex and medulla. Since the cells of the Proximal Convoluted Tubule, or PCT, are highly permeable to both solutes and water, the relative osmolarity of the filtrate remains equal to the 300 milliosmole solute concentration of the interstitium. The cells high permeability also accounts for a 65% reduction in filtrate volume. Watch the simulated drop of filtrate as it moves down the descending loop of Henle to the bottom. Notice that the osmolarity of the filtrate increases and the volume decreases. Recall that the cells of this region are permeable to water but not to solute. As the filtrate moves down the tube through regions of higher osmolarity, water diffuses out into the interstitium reducing the filtrate volume by an additional 15%. The solutes remain behind in the tubule and become more concentrated as the filtrate approaches the bottom of the loop. The cells of the thick segment of the ascending loop of Henle are permeable to solute, but not to water, making them function essentially opposite to the cells of the thin segment of the descending loop. As the concentrated filtrate flows up the ascending loop, the cells actively transport solutes into the interstitium causing the osmolarity of the filtrate to fall to less than 300 milliosmoles. Because water remains in the tubule, the filtrate volume remains unchanged. The opposing flow and opposite activities of the descending and ascending segments of the loop of Henle is called the counter current multiplier mechanism. The osmolarity of the filtrate entering the late distal convoluted tubule, or DCT, and cortical collecting duct can be as low as 100 milliosmoles. Recall that in the cells of this region, the reabsorption of sodium ions and water is regulated by the hormones aldasterone and antidiuretic hormone. In normal hydration conditions, low levels of both hormones promote the reabsorption of sodium ions and water from the filtrate. This maintains the low osmolarity of the filtrate while reducing its volume by an additional 15%. The osmotic gradient constructed by the counter current multiplier mechanism concentrates the urine by drawing water from the filtrate as it travels through the medullary collecting duct. However, the degree of concentration is regulated by antidiuretic hormone, which controls the water permeability of the duct. As seen earlier in this topic, ADH levels vary in response to various conditions including the individual’s hydration status. Let’s observe the normal level of hydration first and then compare that condition with the other two hydration levels. Notice the effect of each condition on the drop of filtrate traveling down the medullary collecting duct. With normal hydration and levels of ADH, water channels are present in the luminal membranes of these cells resulting in moderate water permeability. ADH also facilitates the diffusion of urea out of the medullary collecting duct into the interstitium. Although it is considered a nitrogenous waste product, urea is responsible for up to 40% of the medullary interstitial osmolarity. From the interstitium, urea passively reenters the filtrate in the loop of Henle and recirculates back to the collecting ducts. It may then again diffuse into the interstitium or pass into the renal pelvis as a component of urine. Notice that, as it descends, the filtrate drop shrinks in volume and darkens slightly as water is lost and solutes are concentrated. The filtrate does not equilibrate with the osmolarity of all medullary regions and is therefore not as concentrated as possible. Normal urine has an osmolarity of about 600 milliosmoles or twice normal body osmolarity. With dehydration, a high level of ADH creates two important changes. First, it causes additional luminal water channels to be added to the duct, which increases its permeability to water. Second, it increases the permeability of the duct to urea, which in turn increases the interstitial osmolarity. This increased osmolarity draws additional water from the filtrate. Therefore, as the filtrate passes through the lumen of the duct, it equilibrates with each regional increase in osmolarity. Notice the decrease in size and darkening color of the filtrate drop as it descends through the duct. In severe dehydration conditions, the low volume of urine excreted may be concentrated to about 1400 milliosmoles or more than four times the osmolarity of normal body fluids. With over hydration, ADH levels are very low or absent, and the duct cells remain relatively impermeable to water and urea. The reduction in urea permeability decreases the medullary interstitial osmotic gradiant, reducing the water drawing power of the interstitium. As the filtrate passes through the lumen of the medullary collecting duct, it does not equilibrate with any regional change in osmolarity and therefore remains unmodified. Notice that the filtrate drop remains the same size and color as it descends through the duct. The final urine, which is dilute and high in volume, may have an osmolarity as low as 100 milliosmoles. Now let’s look at the final volume of urine produced per minute and per day for each of the levels of hydration you have just seen. Recall that 95% of the water has been reabsorbed from the 125 ml/min of glomerular filtrate produced by the kidney before the filtrate enters the medullary collecting duct. With high levels of antidiuretic hormone, the approximate final urine volume is 0.2% of filtrate. This is equal to one fourth of a milliliter per minute, or 400 mL/day. Two conditions in which this might occur would be severe dehydration or blood loss. With normal levels of antidiuretic hormone, about 99% of the filtrate is reabsorbed into the blood. These leaves about 0.9%, or 1.1 mL/min, of concentrated urine to continue the passage into the renal pelvis and urinary bladder. This equals about one and one half liters per day. With low levels of antidiuretic hormone, the approximate final urine volume is 12.5% of the filtrate. This is equal to 16 mL/min, or 22.5 liters per day. This situation might be caused by either temporary or chronic conditions. High volumes of dilute urine are temporarily produced after a person drinks either a large volume of fluid or fluids that contain diuretic drugs, such as caffeine or alcohol. In a chronic condition called diabetes insipidus, urinary volume may reach extremely high levels because either antidiuretic hormone is not released by the posterior pituitary, or the tubular cells do not bind in respond to this hormone.
25. The Urinary System
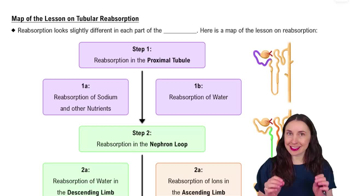
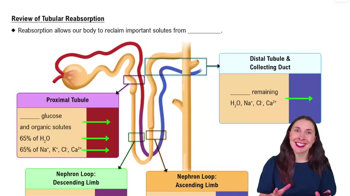
Renal Physiology Step 2: Tubular Reabsorption
Related Videos
Related Practice
 4:06
4:06